What is SEE++



|
What is SEE++ |
|
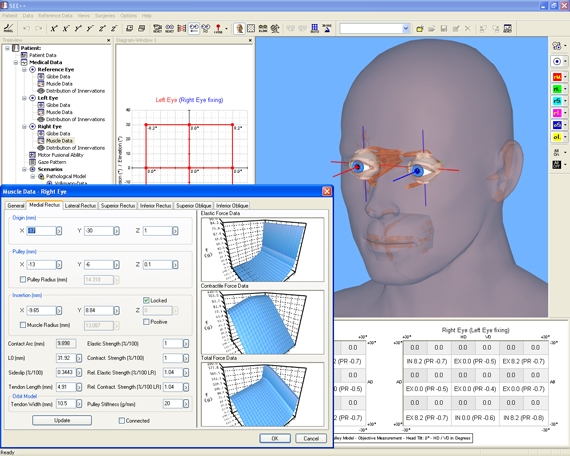
SEE++ is a new simulation system for the prediction of clinical surgery results as well as for the illustration of pathological situations in the field of strabismus surgeries. The system is based on a highly developed mathematical simulation model (biomechanical model). It simulates the behaviour of the human eye together with the extraocular muscles in a realistic way and therefore provides an experimental platform for the simulation of pathologies and the evaluation of possible surgical treatments.
SEE++ is a biomechanical system for the interactive three-dimensional simulation and visualization of eye motility disorders and their surgical correction.
SEE++ offers:
•compact, descriptive and thus well understandable knowledge transfer in teaching and training,
•scientifically oriented procedures,
•exploration of basic principles supported by numerous examples,
•a basis for individual considerations of diagnostics and surgical correction of eye motility disorders.
SEE++ is suitable for many people:
•Ophthalmologists, specialists as well as orthoptists can use SEE++ to support measurements and to archive pathologies and treatment methods.
•Researchers in the field of ophthalmology, strabismology and neurology, pediatrists as well as researchers in the field of biophysics use SEE++ as an extensive scientific tool for the investigation of the mechanics of eye movements.
•SEE++ offers a substantial support to teachers through descriptive representation for understanding eye movements. Students have the possibility to interactively deepen their knowledge about (previously studied) fundamentals of eye movement and strabismus.
SEE++ is a Biomechanical Model
The interdisciplinary research area of biomechanical modeling deals with the computer-aided modeling of anatomical structures of the human body. The research project SEE-KID (Software Engineering Environment for Knowledge-based Interactive eye motility Diagnostics) presented here focuses on the virtual representation of the oculomotor apparatus in terms of a functional model of eye motility for the application in the field of ophthalmology.
Looking back on the history of the development of models in the field of strabismus, the strong mathematical implication and the multidisciplinary complexity of this subject area can be noticed. Especially in teaching and training in the field of ophthalmology a detailed understanding of the mechanics of eye movements as well as the functional connections of the anatomy of the oculomotor apparatus with regard to diagnosis and therapy of eye motility disorders is of major relevance. The computer-aided simulation system SEE++ presented here enables the doctor to simulate pathological situations with the computer, to visualize them graphically and interactively in a three-dimensional way as well as to calculate the effects of eye muscle surgeries in comparison to a selected standard model. Thus the surgeon can observe the trend of an eye muscle surgery already on the computer and determine the respective optimal treatment for a patient. By modeling and simulating eye motility disorders with the help of a model and by getting a deeper understanding of the underlying mechanism, multiple surgeries could be avoided.
Biomechanical modeling is defined as a subsection of mechanics. It deals with the effects of dynamical force relations of the human body. The basis for the implementation of such models is the combination of disciplines of physics with fields of biology and physiology. In the broadest sense, studying mechanical properties of the human body with the help of mathematical-physical methods can also be assigned to the new scientific discipline of bioinformatics.
Modeling of the oculomotor system is based on detailed knowledge of anatomical structures and was already described in first simple models in the 19th century. Volkmann was the first to perform extensive measurements of insertions and origins and to determine a detailed description of the geometry of extraocular muscles. Later, Krewson described the geometrical principles of ocular movements in a very simplified form by inventing the so-called "string model". Boeder transformed the mathematics of the string model into a graphically descriptive notation (muscle force distribution diagrams), which is still used in clinic and science today. The first model, which also considered movement-restraining structures of eye muscles, was published as "tape model" by Robinson in 1975. A mathematical reinforcement of this interpretation of muscle fixation led to the definition of the "intensified tape model" by Kusel and Haase in 1977. With the discovery of pulleys as functional elements, a new, advanced model of ocular motility called Orbit™ was introduced as the first commercially available biomechanical eye simulation by Joel Miller in 1994 (see [Miller 1999]), which, compared to older models and clinical data, supplied substantially more realistic predictions.
However, latest studies have shown that pulleys do not only determine and stabilize the muscle path, but that also the pulley position slightly changes with the gaze position. Thereby, the direction of pull of the eye muscles is affected, which can be seen by the bending of the muscle path in different gaze positions. Demer et. al. showed in a study that the pulley position moves backward when an eye muscle is contracted and forward during relaxation. This is called the "anterior – posterior shift" of pulleys. This so-called "Active-Pulley-Hypotheses" is also supported by other studies and was realized in the SEE++ system in form of the active pulley model. Consequently, SEE++ is the first simulation system that implements the "Active-Pulley-Hypotheses".
For the quality of a biomechanical model, characteristics of clinical results and dynamic expandability are of greatest importance. An existing model cannot be considered relevant unless the functional characteristics correspond tendentiously with clinical experiences. Furthermore, the model structure should be arranged in such a way that the incorporation of new physiological or biological findings will not invalidate the behavior of the current model formulation. In order to be able to realize such structures in a computer-aided model, additional methods of software engineering need to be applied.