Strabismus



|
Strabismus |
|
Every permanent or regularly occurring misalignment of the eyes is described as squinting ("Strabismus"). Thereby the eyes are not parallel, but one eye diverges from the gaze direction of the other. About 6% of our population suffer from some form of strabismus. They suffer not only from the frequently disfiguring externally visible abnormality, the visual impairment associated with squint is an even greater burden. Squint is not just a blemish but often a severe visual impairment. The earlier squinting occurs in a child's life and the later it is treated by an ophthalmologist, the more serious the visual impairment will get. With the beginning of school age, the chances of success for the treatment significantly decrease. Squinting babies and infants therefore require a treatment as early as possible.
The Development of Visual Acuity
Babies are able to perceive their environment through their eyes quite soon after birth - but only indistinctly. In the first six months of life they learn to fixate with their eyes and to coordinate their eye movements. During this time of practice, occasional disorders of the eyes are still normal (so-called "baby squinting"). If, however, after the first sixth month of life one eye still deviates from the gaze direction of the other eye, an ophthalmologist should be consulted. In general, an examination of the eyes directly after birth would make sense to correct any disorders, e.g. a congenital cataract, at an early stage in the first weeks of life.
Visual acuity of infants improves continuously in the course of growth. By the time school age is reached, the eyes' learning program is virtually complete. The correction of amblyopia as a consequence of strabismus is only possible during this sensitive development phase. Already from the 7th-8th year of life the chances for a normalization of the visual acuity decrease seriously. After the 10th-12th year of life they are almost zero.
The Various Forms of Squinting
When squinting is present, one or sometimes both eyes deviate from their common gaze direction. If always the same eye is squinting because it has the poorer visual acuity or restricted movability, this is referred to as one-sided ("mono lateral") squinting. If, on the other hand, the deviation alternates between the right eye and the left eye, this is called alternating squinting. Occasionally, the deviation is so marginal (less than 5 degrees), that it is scarcely noticed. In this case one speaks of micro squinting, which normally is an inward squinting on one side and so marginal that parents do not recognize it or even think it looks cute. If a deviation in any direction can practically always be observed, it is referred to as manifest squinting. Occasionally, squinting can only be observed, if the binocular vision is restricted by covering one eye (Cover test). In this case one speaks of a hidden ("latent") squinting, which is fully or partially compensated through an adequate fusional effort. This often leads to headache, reading problems etc. (asthenopic disorders). Squinting is never harmless or simply cute. It also "does not heal while growing up", but often causes amblyopia of one eye and serious disorders of the binocular and mainly of the high-quality three-dimensional vision, if the necessary ophthalmological treatment is delayed.
The squinting eye can deviate from the non-squinting eye in different directions: inwards (esophoria), outwards (exotropia), upwards (hyperphoria) or downwards (hypophoria). Sometimes a child suffers from deviations in different directions at the same time.
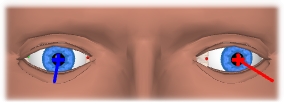
Inward Squint (Esophoria)
|
Outward Squint (Exotropia)
|
How Does Squinting Emerge ?
The causes of squinting are multifactorial. The fact that squinting occurs frequently in some families implies congenital factors. Particularly if one or both parents were squinting or were treated because of squinting, the child should have an ophthalmological examination right in the first year of life and every year later on. Further factors that can cause squinting and amblyopia are a pregnant mother's infection with rubella or premature birth. In most cases the causes can be found at the eye itself, such as a congenital refractive error (like hypermetropia or a serious corneal curvature) or a partial cataract, tumors inside the eye or injuries of the eye.
In case of congenital causes, the motility disorder isn't always obvious immediately after birth. In case of congenital refractive errors, squinting doesn't emerge until the child begins to fixate more accurately. In doing so the child often exclusively uses the functionally better eye, and so the more ametropic eye develops an amblyopia, if it isn't "trained" by therapeutic treatment. Sometimes an "acquired" disorder also suddenly appears, e.g. after children's diseases, after high fever, after accidents or in phases of serious psychological strain. Then latent strabismus is uncompensated due to an abnormal event.
Is There an Early Stage Indication for Squinting ?
Children with conspicuous strabismus have the best chances, because their parents will take them to the ophthalmologist early enough due to the "blemish". But unfortunately there also exist scarcely visible or invisible strabismus defects (micro strabismus). In case of latent strabismus, there are sometimes indications for decompensation due to manifest strabismus, e.g. occasional narrowing of one eye, sensitivity to light etc. A head posture is also common with nystagmus. But quite often children behave in an absolutely normal way and a visual impairment is first diagnosed in a serial examination in nursery, when one eye is already amblyopic and an effective treatment becomes difficult.
How Does Squinting Affect Vision ?
For three-dimensional spatial vision, both eyes must exactly fixate an object of interest. The image of this object is then projected onto the yellow spot (fovea), the center of sharpest vision, of both eyes. So, for example, a cube fixated with both eyes is projected upside down (like in a camera) and perspectively slightly different for each eye (due to the interpupillary distance of the eyes) onto the retina. In the brain, both images are merged in order to perceive one upright three-dimensional cube (fusion) (a).
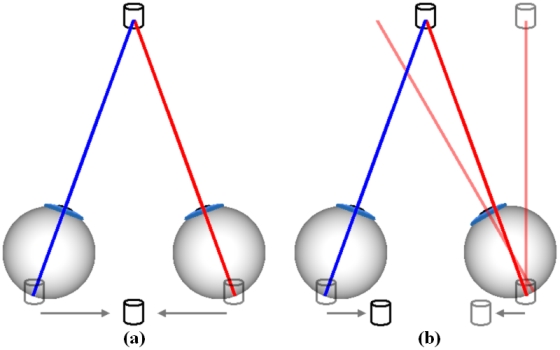
This is different for an inward squinting of e.g. the right eye. According to this, the right eye fails to fixate the cube and misaligns as compared to the left eye (b). Different images are now projected onto the fovea of both eyes, and the brain fails to merge this information. The result is, that disturbing (uncrossed) double images are perceived. Especially in infants, the brain will compensate these errors by trying to eliminate those images that originate from the squinting eye. This process leads to a fatal outcome: the squinting eye will lose visual acuity and will suffer from amblyopia.
Amblyopia is referred to as a functional deficiency of visual acuity of an otherwise healthy eye, caused by e.g. squinting.
Without proper treatment, almost 90 % of all squinting children develop a one-sided amblyopia. The magnitude of the angle of squint is thereby negligible: especially in case of micro strabismus, amblyopia has a distinct tendency. If this amblyopia due to squinting is not discovered and treated early enough, it remains lifelong. Then the child can never learn how to see with both eyes or how to correctly see in a three-dimensional way. It is more at risk to get hurt in accidents and furthermore hindered in the freedom of choosing a career. A timely treatment can prevent an amblyopia due to squinting and can often establish limited binocular vision and also good three-dimensional spatial vision.
How Is Squinting Treated ?
The primary goal of treatment is to achieve the best possible binocular visual acuity (eyeglasses!). Only then a strabismus surgery with normal interaction of both eyes can be successful and enduring. Eyes without fixation (e.g. blind eyes) do not keep the parallel position after a strabismus surgery in most cases!
1) Eyeglasses
A not corrected ametropia can cause strabismus. Many children in Europe who suffer from strabismus are hyperopic. Excessive near fixation (accommodation) can result in squinting for these children due to the convergence impulse. Hyperopic eyeglasses, which are adjusted during a complete relaxation of accommodation by using eye drops, can therefore "heal" this type of accommodative strabismus or at least minimize the squint angle.
2) Covering ("Occlusion")
Occlusion of the normal eye is used to eliminate the amblyopia of the squinting eye. At the same time the eye muscle activity of the squinting eye is improved. A manifest squint angle cannot be corrected with this procedure, it can even increase.
According to the ophthalmologist's instructions, adhesive plasters are stuck over the normal and occasionally also over the squinting eye in a specific changing rhythm. This is done in order not to endanger the normal eye. If a child does not tolerate the plaster treatment, eye drops are prescribed. The eye drops widen the pupil of the normal eye and do not allow it to focus, especially in the near distance, anymore. Therefore, the child is forced to use the predominantly squinting, weaker eye and to "train" it that way (penalization).
If a certain visual acuity is reached, vision occlusion plasters are used. These are fixed onto the eyeglasses. The amblyopia treatment with such plasters often has to be discontinued "gradually" over years until adulthood in addition to eyeglasses and even after successful surgery.
3) Squint Surgery and Subsequent Treatment
The disorder of squinting children often has to be corrected through surgery of the outer eye muscles. Normally this is not done until the child has reached an approximately equal vision by the use of full-corrected eyeglasses. The strabismus surgery reduces or eliminates the squint angle. The postoperative wearing of glasses is still necessary. Furthermore, often an occlusion in terms of e.g. a part-time occlusion is necessary until adulthood.
Strabismus surgeries are normally low-risk surgeries and have good chances of success. They are performed on children in general anesthesia, that means that after a sedation, the "sedative injection" or the suppository and the initiation of the narcosis the child does not notice anything of the surgery.
The surgery is carried out by opening the conjunctiva in order to reach the extraocular muscles.
The operated eye is slightly reddened postoperatively. The child reduces the eye movements for approximately one day postoperatively. If a second surgery is necessary depends on the type of disorder and on the size of the squint angle.